Understanding the Differences: Mini, Traditional, Extended, and Circumferential Tummy Tucks
Tag Archives: abdominoplasty
As a board-certified plastic surgeon, I, Dr. Sam Jejurikar, perform a high volume of tummy tuck procedures, helping patients achieve a flatter, more contoured abdomen. I’m fortunate to have been selected to D Magazine’s Best Doctors list for the past five years and Newsweek’s Best Plastic Surgeons list for the past three years. When considering a tummy tuck, it’s important to understand the different options. What are the differences between, mini, traditional, extended and circumferential tummy tuck? The main difference between each type is incision length, but all allow for muscle tightening (rectus plication) and liposuction to enhance results.
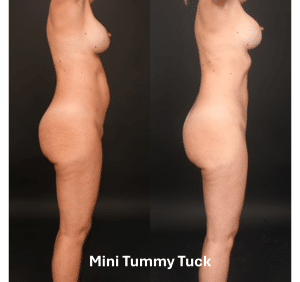
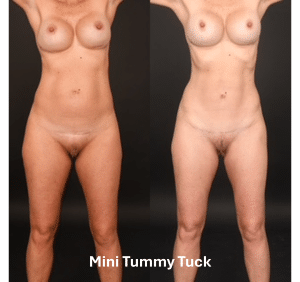
Mini Tummy Tuck: Subtle Enhancement with a Small Incision
A mini tummy tuck is ideal for patients with mild skin laxity below the belly button. The incision is short, similar to a C-section scar. This procedure removes excess skin, tightens lower abdominal muscles, and preserves the belly button. While there’s no incision around the belly button, I can perform an umbilical float (navel repositioning), slightly lowering it for a more natural result.
Ideal Candidate:
✔ Mild skin laxity below the navel ✔ Shorter recovery than a full tummy tuck ✔ Close to ideal body weight with limited need for skin removal
Traditional Tummy Tuck: Comprehensive Abdominal Rejuvenation
A full tummy tuck removes excess skin and tightens muscles from the ribcage down to the pubic area. The incision runs from hip to hip but stays low enough to be hidden by most underwear and swimsuits. The belly button is repositioned, ensuring a natural appearance. While this procedure dramatically tightens the front of the abdomen, it does not provide as much contouring to the sides or waist.
Ideal Candidate:
✔ Excess skin and muscle laxity after pregnancy or weight loss ✔ Desire for a flatter, firmer abdomen ✔ Needs full rectus muscle repair but not much lateral contouring
An extended tummy tuck goes beyond the traditional approach by removing excess skin that extends past the abdomen to the sides of the waist. The incision reaches beyond the hip bones, allowing for enhanced sculpting of the flanks and waistline. This procedure is excellent for patients seeking a dramatic hourglass figure and greater definition beyond the front of the abdomen.
Ideal Candidate:
✔ Loose skin extending past the abdomen ✔ Desire for more contouring along the waist and hips ✔ Desires dramatic reshaping of body to create an hourglass silhouette
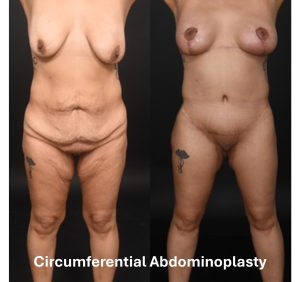
Circumferential Tummy Tuck: 360-Degree Contouring with Gluteal Enhancement
A circumferential tummy tuck, also called a body lift, removes excess skin from the abdomen, sides, and lower back. The incision extends around the entire waistline, providing a full 360-degree transformation. In addition to creating a flatter, firmer midsection, this procedure allows for gluteal autoaugmentation, where excess tissue from the lower back is used to naturally enhance the buttocks. This option is especially popular among patients who have experienced massive weight loss.
Ideal Candidate:
✔ Significant skin laxity in the abdomen, back, and flanks ✔ Desire for full lower body contouring ✔ Interest in a natural buttock enhancement through autoaugmentation ✔ Stable weight after major weight loss
Choosing the Right Tummy Tuck
The best procedure depends on how much excess skin you have, muscle separation, and your overall goals. I perform muscle tightening and liposuction with all tummy tuck procedures to achieve the best contour possible.
If you’re considering a tummy tuck, I’d love to discuss your options. Schedule a consultation by calling us at 214-827-2814 to create a customized plan for your transformation.
Liposuction is one of the most effective procedures for removing unwanted fat and reshaping the body. However, not all fat is created equally, and the presence of visceral fat can significantly impact the results of body contouring surgery. I frequently encounter requests to perform liposuction on individuals with significant amounts of visceral fat. I must explain to these patients that surgical intervention is not a viable option for treating such fat deposits. Understanding the anatomic location and health implications of visceral fat, its limitations in optimizing the results of surgical procedures, and how to reduce it is essential for both patients and surgeons alike.
Visceral Fat
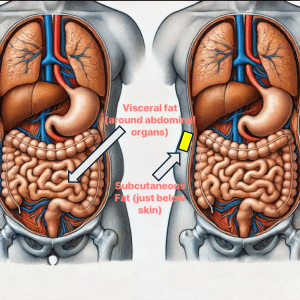
What is visceral fat? Fat in the human body is classified into two main types: subcutaneous fat and visceral fat.
Subcutaneous fat is the soft, pinchable fat that lies just beneath the skin. This is the type of fat that can be effectively targeted and removed through liposuction.
Visceral fat, on the other hand, is stored deep within the abdominal cavity, surrounding internal organs such as the liver, intestines, and pancreas. Unlike subcutaneous fat, visceral fat cannot be removed through liposuction due to the high risk of perforating the gastrointestinal tract or damaging solid organs.
Why Is Visceral Fat a Concern for Body Contouring Surgery?
Patients seeking body contouring procedures, such as liposuction or abdominoplasty, often expect dramatic results. However, the presence of excessive visceral fat can limit these outcomes for several key reasons:
Inability to Remove Visceral Fat with Liposuction: Liposuction exclusively targets subcutaneous fat, as it involves suctioning fat cells from directly beneath the skin. Visceral fat, which is located inside the abdominal cavity, is inaccessible to liposuction techniques. No surgical method can safely remove visceral fat directly, meaning that patients with a high volume of visceral fat will not achieve the slimmed-down look they desire after surgery.
Impact on Abdominal Contouring: Patients with excessive visceral fat will still have a convex abdominal shape after liposuction. This is because the fat pushing outward from inside the abdominal cavity remains unchanged. While liposuction can remove superficial fat and improve body contour, it does not address the deep-seated fat responsible for a bloated midsection.
Increased Surgical Risks: Excess visceral fat is associated with a range of health risks, including insulin resistance and type 2 diabetes, high blood pressure, and cardiovascular disease. From a surgical standpoint, patients with excessive visceral fat may face increased risks of complications such as poor wound healing, infections, and prolonged recovery times.
Affects Muscle Tightening Procedures: In cases of tummy tuck (abdominoplasty), surgeons not only remove excess skin but also tighten the abdominal muscles to enhance contouring. However, significant visceral fat can put pressure on these muscles, making it more difficult to achieve optimal tightening and a flat abdominal profile. This means that even with muscle repair, the desired abdominal flattening may not be fully realized.
How to Reduce Visceral Fat Before Surgery
Because visceral fat cannot be removed surgically, patients must take steps to reduce it through lifestyle modifications. Some effective ways to reduce visceral fat include:
Adopt a Healthy Diet: Focus on a high-protein, low-carb, and fiber-rich diet to promote fat loss. Avoiding processed foods, excess sugar, and trans fats can help reduce visceral fat content over time.
Exercise Regularly: Engaging in cardiovascular exercises, such as running, cycling, or swimming, helps burn visceral fat more effectively than spot-reducing techniques.
Strength Training: Incorporating weightlifting or resistance training into your routine can boost metabolism and promote overall fat loss.
Manage Stress and Sleep: Chronic stress and poor sleep are linked to increased visceral fat accumulation. Practicing stress-reduction techniques and maintaining proper sleep hygiene are vital in promoting fat loss.
Medical Interventions: For some individuals, GLP-1 agonists (such as Mounjaro or Ozempic) or other medically supervised weight-loss treatments may be recommended to help reduce visceral fat before undergoing surgery.
Who Is an Ideal Candidate for Liposuction?
The best candidates for liposuction are those who:
Have realistic expectations about what liposuction can and cannot achieve.
Are at or near their ideal body weight with minimal visceral fat.
Maintain a healthy lifestyle with balanced nutrition and regular exercise.
Have good skin elasticity, which allows for better contouring post-surgery.
Final Thoughts
Liposuction is a powerful tool for refining body shape, but it is not a solution for deep, visceral fat. Patients must understand that visceral fat reduction requires lifestyle changes, and achieving an optimal body contour involves a combination of surgery and personal health management. By taking proactive steps to lower visceral fat before surgery, patients can improve both their surgical results and their overall health. If you’d like to learn more, do not hesitate to reach out to my Dallas Plastic Surgery office (Dr. Sam Jejurikar) at 214-827-2814.
Dr. Sam Rhee: Hello and welcome to Three Plastic Surgeons and a Microphone, as always joined by my fellow colleagues, Dr. Sal Pacella in La Jolla, California. His Instagram handle is San Diego, the plastic surgeon. Dr. Sam Jejurikar is in Dallas, TX; his Instagram handle is Dr. Sam Jejurikar, and I am Dr. Sam Rhee in Amos, New Jersey. And my Instagram handle is at Bergen Cosmetic.
Today we are going to be talking about abdominoplasty. Our last episode was almost a year ago, and it was one of our most popular episodes. And it’s one of those topics that many people have a lot of interest and questions about. So we’re definitely going to take a deeper dive into it today and talk a little bit more about it. But first, as always, we have our disclaimer.
Dr. Salvatore Pacella: This show is not a substitute for professional medical advice, diagnosis, or treatment. This show is for informational purposes only. Treatment and results may vary based on the circumstances, situation, and medical judgment. After appropriate discussion, always seek the advice of your surgeon or other qualified health provider with any questions you may have regarding medical care. Never disregard professional medical advice or delay seeking advice because of something in this show.
Understanding Tummy Tuck Options: Liposuction vs. Abdominoplasty
Dr. Sam Jejurikar: And I will lead the discussion today, gentlemen. As Sam had mentioned, our last episode on tummy tuck was one I had gotten the most questions and comments about from viewers, so we thought we would revisit it. I generally have found, and tell me if you disagree with me. Most people don’t want a tummy tuck. That’s not a thing that anybody ever comes in and says, Dr., I really want a tummy tuck. But it’s a thing that people are generally reconciled towards.
So I thought the way we would lead the discussion today was I would show you a case and then ask you a bunch of questions. So this lovely woman is in her mid-30s and has three kids. She says she’s a little overweight. She wants to lose about 20 or 25 pounds. She doesn’t like the way her tummy looks. We also talked about her breast and did some stuff on her breast. But we’ll leave that out of today’s discussion. But just wants to know, Dr. Pacella, do I have to have a tummy tug? Can you just do liposuction on me and make me look better?
Dr. Salvatore Pacella: It’s a very common question we get, and what I tell patients is, well, two things. Number one is there are different two different positions where the fat could be on your belly. There’s external fat, and then there’s internal fat. Right? And so that, wow, perfect set up here. Wow! It’s like…
Dr. Sam Jejurikar: If we coordinated this.
Dr. Salvatore Pacella: And often patients, I think, sometimes have some difficulty articulating or understanding this. Those patients have a lot of intra-abdominal fat, and they are probably at least moderately overweight to start with. A tummy tuck will have a very challenging result to look good because that intra-abdominal fat cannot be compressed, one thinks. And so the protuberance of this fat oftentimes just doesn’t create a very nice, natural hourglass shape.
So patients who are more amenable to getting their cosmetic results from a tummy tuck oftentimes have a lot of external fat and skin compared to internal fat. The second most important thing that I tell patients is that skin consistency with that external fat is very important. So let’s go back to your previous patient here.
So, looking at her now, obviously, without doing a physical exam on her, her belly is not massively perturbed by any means, and she does have some adiposity or some fatty tissue on her love handle area. And centrally, I think with this patient, I certainly would have a discussion about potentially just using liposuction, particularly over the front and sides of the belly.
But I will qualify that by saying it’s not going to do much for your skin. Your skin has decent consistency and elasticity; it may contract a bit, but if you want the tightest look possible, a tummy tuck will do it.
Dr. Sam Jejurikar: What about you, Dr. Rhee?
Dr. Sam Rhee: I think Sal hit the nail on the head, and you said it too, Sam. People don’t come in saying, give me a large incision right down there on my belly. You’re right; nobody actually comes in. Very few actually come in asking for that. So when you have a patient, and I’ve had patients very similar to ones that look like this, who say, you know what, I don’t want that cut. Can you just do liposuction for me? I don’t want anything else.
I’ll have that discussion that Sal just had with that patient, and it’s really about trying to accommodate that patient but also letting them know what the potential consequences are as well. I think that’s a give-and-a-take that you always have with every patient, and you sort of have to work with them. Liposuction only removes fat. If you have to remove the skin, you’re going to have to make a cut somewhere on the body. That’s just the physical truth, and you have to talk to the patient about that.
Dr. Salvatore Pacella: Yeah, I would say in this particular patient, again, it’s not super detailed; there’s a little pixelation. But suppose that skin has decent elasticity and stretches a bit. In that case, I might consider simply doing liposuction with maybe what I call a mini tummy tuck, which is removing a small amount of skin inferiorly. And I think if the patient is not keen on the idea of a big, massive incision or the big recovery associated with a tummy tuck, and she realizes that it’s not going to get nearly as tight, that may be a decent option, a little mini abdominoplasty with some anterior liposuction.
Dr. Sam Jejurikar: So in that scenario, Sal, which I think is very reasonable. What would you do with her muscles? Because when you look at this, particularly the lower portion of her tummy, there’s a little poop. Would you placate the muscle, which tightens the muscle? The people don’t know what that word means, or would you just leave it alone?
Dr. Salvatore Pacella: Yeah, so good question. It’s obviously hard to see just on the photograph, but that will be one thing I’m going to be absolutely looking for on my physical exam. So in this particular patient, to me, this almost looks like that’s a fatty deposit versus a rectus diet.
Dr. Sam Jejurikar: I’ll tell you, it’s rectus. {Crosstalk}
Dr. Salvatore Pacella: Got it. Okay. Alright. So if that area was simply fat, it’s amenable to liposuction. But if we’ve got some pooch and some muscle in a mini tummy tuck, there’s only a limit to the amount of placation you can do, and you can only really do it on the lower portion. So I would be very conservative on that. And it begs the question if we’re going to tighten up the abdominal wall muscles anyway, why not just do the full monty? That’s where the recovery comes in. The recovery comes in and sewing the muscles.
Dr. Sam Rhee: I was just going to add that if you do the plication of the lower part of the belly, you can make the upper part look worse. So I agree with Sal. You got to sort of be careful with that.
Dr. Sam Jejurikar: Well, I’ll jump ahead a bit here. So she told me, Dr. J, I want my tummy to be as flat as possible, and I want to lose some weight. I want to lose, like, 25 pounds, 30 pounds. Should I lose that weight before or after I have the procedure? What would your guy’s answer to that question be? How much do I have to lose at all?
Dr. Sam Rhee: For me, I don’t think I’ve seen very many patients. They all have goals of losing 20 to 30 pounds. It’s always a little aggressive. I don’t know if I’ve ever actually seen it. I’ve seen very few, maybe a few, but not that many actually lose that weight beforehand. I usually ask them what their happy weight is. If it’s 20 or 30 pounds below whatever they are now, I’ll say, you know what? We’re good if you get to within five to ten of that happy weight.
Dr. Sam Jejurikar: What about you, Sal?
Dr. Salvatore Pacella: I would say it’s always best to lose as much weight as you can prior to surgery. But like Sam, I think it’s rare that anyone can achieve a consistent goal of losing the 20 pounds they put out to. And if I can get half of that, I’d be happy.
Effective Scar Management Techniques for Tummy Tuck Patients
Dr. Sam Jejurikar: I typically tell people something very similar to what you guys just said: to get within 10 to 15 pounds of your goal weight. That’s pretty good. If you can do that. I think there’s a hypermetabolic state that happens with surgery. You lose some weight with surgery, and all is said and done. And I think when you settle out, you’ll be pretty good. So she did lose a little bit of weight before you see these postop pictures, but about 15 pounds probably, and it loosened up the skin more.
So the conversation about a mini tummy tuck became less of an issue. So then the next thing we had a conversation about, because she had a bunch of concerns, was a scar. As both of you have said, nobody wants that scar, but eventually, if you’re bothered enough by the appearance of your tummy, you’re reconciled to it. But she said I want to do everything I can about the scar. Tell me what your protocol is to make my scar look as cosmetically acceptable as possible. How would you answer that question? Is either one of you?
Dr. Sam Rhee: Go ahead, Sal.
Dr. Salvatore Pacella: I would usually say so. The first thing is really on me: when I repair this in the operating room, I want to repair the skin under minimal tension, if any. I want to close this in multiple layers. I want to make sure that we’re not getting an infection. We will use monofilament sutures so that we don’t have spitting incisions, etc. And then, after surgery, the things that patients can do is I tend to use a lot of silicone ointments and a lot of adjuvant scar treatments, such as laser if needed.
So there are multiple things we can do afterward to improve the scar. And I think the key is patient expectations and education that the scar will probably look the worst in about three months. This sort of second phase of wound healing causes a lot of redness, but that slowly fades after about eight to twelve months. So I think patients’ expectation is just as important.
Dr. Sam Jejurikar: And Sam.
Dr. Sam Rhee: Yeah, I can’t remember who said maybe it was Kuzan at Michigan who said scars. The appearance of scars is a combination of a couple of things. One is genetics, the second is how the scar is made, and the third is how you manage the scar afterward. And so all those three things do play a role. As Sal said, the one that we control is the actual incision and how we put it together and close it. And any plastic surgeon who’s worth their salt is going to do a good job with that, or at least the best that they know how.
And then, you talk to the patient based on who they are. I have a lot of patients who are Latinx or African American, who have a lot of concerns about scarring, so we’re really vigilant afterward. We do the same things that Sal talks about. I’ll start with silicone gels really quickly. We monitor very diligently, and we intervene early if we have to. Those are the things that help minimize scarring in most patients.
Dr. Sam Jejurikar: Yeah, what I would say is the last time we did this, Sal made a point, which he didn’t make this time, but is so true, which is the meticulous closure that you do. One of the things that Sal mentioned that he did last time is that he does running closures of the deeper layers to offload tension. Wasn’t that you, Sal, that said that you actually do a running scarf as fascia closure?
Until that episode, I have largely been doing an interrupted closure. But I adopted that after we did that episode, and it’s made a huge difference. It has actually made the consistency of the scars actually better. So I want to thank you for that. That’s a huge point, though; surgeons should be doing everything they can to offload tension on the closure to make the scars look as good.
The other thing that both of you said, which I 100% agree with, was you both mentioned silicone. I think silicone, and there are other adjuncts that I want to ask you about in a second. But I think silicone, either in the form of strips or gels, is the gold standard for scar care. How long do you tell your patients they should be using it after surgery? Because I’ll typically get people that will use it for a few weeks and say it doesn’t work and then just stop using it. What do you tell them upfront about how long they need to be taking care of their scars?
Dr. Salvatore Pacella: Six months.
Dr. Sam Rhee: I said six months. Yes, exactly six months. But honestly, I’ll be lucky if I get half that in a lot of patients.
Dr. Sam Jejurikar: Yeah, I tell them a year. I tell them they need to be babying their scar and obsessing over it for over a year. Let’s say you have them doing silicone, and their scars are looking okay, but they’re still a little bit thicker and a few months out. What other things do you tell people are useful for their scars? Postoperatively? Do you think micro-needling, for instance, is useful for scars? Do you think lasers are useful for scars? Do you do steroid injections?
Dr. Salvatore Pacella: I definitely think the laser is a key component. I work very closely with a cosmetic dermatologist, and the blade of lasers can really tremendously help with the appearance of scars early on. Throughout my career, I’ve really gotten away from injecting scars with silicone. I’m sorry. Kenalog or Steroid. And I have just found that it is so inconsistent and doesn’t distribute through the scar very easily.
There are oftentimes pockets of white material when you try to inject it. It’s just very challenging. I will say, though, I know this discussion is about abdominal plastic, but in the face, I’ve been starting to use a lot of five FU injections, particularly around the eyelid, which I find much easier to inject. It can be very effective in breaking up scars. I haven’t done it in a larger scar, though.
Dr. Sam Rhee: We all have our preferences. If I see any sort of scar or hypertrophy, I do a combination of topical and Kenalog injections. For me, it works pretty well. I mean, it’s not that often that I have to get to that point, but that’s something that I’ve sort of done for a while, and I’m okay with it. I agree that it is a little inconsistent.
I will probably have to see the patient back in about six weeks and see how they’re doing with it. When I first started doing that, maybe 10 or 15 years ago, I don’t know what I was doing back then. I don’t remember. But I overdid it. I way overdid it, and I had issues with that. Now I don’t know. I guess it’s experienced for me that just doing it, I tend to know what I can do with it, and just sort of it seems to work for me as long as I keep a close eye on it.
Dr. Sam Jejurikar: It’s very interesting listening to the two of you because I couldn’t agree more. I think that less is more where Kenalog is concerned. I use it a bit, but I have realized it’s a dilution, and the amount needs to be much less than I did earlier. I also think there’s a role for micro needling for scars that are thick. It’s actually easy to do. I’ve seen it lead to some remodeling of thicker scars in darker-pigmented patients.
I like bleaching creams a lot, hydroquinone creams. I think they help a lot with some of the dark brown discoloration that you see in lighter skin patients. I like broadband light treatment discoloration, but I think there are a lot of things that you can do. I think the great thing is seeing how you guys have relationships with people that are cosmetic dermatologists. We have a skincare center.
Finding someone who is passionate about treating that and having the right amount of time can lead to some good results with scars. The next question, though, that she had for me is, Dr. J. I want to know if you’re going to do any liposuction at the same time you do my tummy tuck. And how would you guys answer that question? And if so, where would you do liposuction on this patient? I’ll go back to her pictures.
Dr. Salvatore Pacella: Yeah, absolutely. I think for every single abdominal plastic I do; I add liposuction to at least the love handle, kind of lower back, flank area, and many times along the hip. I think that is crucial when I think about abdominal rejuvenation. We really want to do a 360-degree rejuvenation. If you tighten up the tummy muscles, tighten up the skin, and then you got this kind of muffin top on the side, nobody’s happy with that, right?
Definitely add some liposuction. Now the question becomes, how do we incorporate liposuction into the actual procedure on the front of the tummy? And that’s something that I think has evolved tremendously in my practice over the last several years. For example, another beautiful segue here.
Dr. Sam Rhee: I know.
Dr. Sam Jejurikar: Hand drawn by me this morning. Thank you very much. Yeah.
Liposuction and Swelling Management in Tummy Tuck Procedures
Dr. Salvatore Pacella: So traditionally, in plastic surgery, it was a serious faux PA to liposuction. Anything on the abdominal plastic skin flap, and I think philosophy is changing as long as you’re not super aggressive. So, for example, at the upper portion of the chest on the upper abdomen, many patients have some fatty rolls here, right up above the rib cage area, and that can sometimes be problematic if we don’t hit that a little bit with some liposuction. The other place I like to do it is centrally in the abdomen. Oftentimes a beautiful abdomen has a little bit of a central dip, so I think that’s a nice place to do it.
Dr. Sam Rhee: I agree 100% with Sal. I do way more liposuction with my tummy tucks now than I ever have in the past. I think we talked about it before. The 360 is super important. The flanks, as Sal said, the back. And yeah, they used to scare us about the upper abdomen when we were learning about this stuff, that you would revascularize the flap. And I guess it’s with the experience again now; I just feel like I can do a much more aggressive job in that area than I used to without having to worry about that sort of devascularization.
Dr. Sam Jejurikar: So this picture that Sal referred to as a nice segue is a modification of the kind of a classic picture that Steve Wallach and Alan Monterosa, both of whom are mentors of mine, did to sort of help define the blood flow to the abdominal wall with liposuction. And so green, basically the love handle area, and you can incorporate the back into it as well, is a safe zone for us to do and feel pretty good about.
You can obviously do as much liposuction as you want to under the skin flap as well that you’re going to take off unless I’m doing fat grafting and I need fat for some reason; I don’t typically do that. But the question sort of becomes a central portion of the abdomen. Yellow is what we kind of view to be a zone of extreme caution around. It’s a little bit less, but we worry about the blood flow.
And so what I’ll often pose to the question is, do you want me to try to hit a home run on your case, or do you want me to hit a single or a double? And what I mean by that is they’re going to look great with the tummy tuck, but to get a sculpted look on the upper abdomen, you have to do some aggressive liposuction. And the potential risk of that is some healing issues.
The healing issues typically happen in the lower portion of the abdomen; it heals. It can be messy for a few weeks and a little disconcerting to people if they get healing issues. But I have found as I have gotten much more aggressive with my liposuction, which I definitely have, the incidence of getting some minor wound healing complications is not insignificant. Have you guys seen that as well?
Dr. Salvatore Pacella: I just haven’t been overly aggressive. I really just limit my liposuction to the upper pole a bit, and then centrally, I rarely go into the areas that are kind of along the central column.
Dr. Sam Jejurikar: Yeah.
Dr. Sam Rhee: For me, it depends if the patient has any comorbidities. I’m pretty conservative, and then I’ll tell the patient sometimes we may have to do a little bit more in the future if there’s an issue; it’s patient-specific. For me, it really just depends on the individual and how much fat there is, to begin with as well.
Dr. Sam Jejurikar: Yeah, it’s the rare patient that I will liposuction the entire upper flap on, don’t get me wrong, but sometimes people are very demanding in terms of what they want and see, they have to understand the risk that goes along with it. I’m not trying to say that everyone should get aggressive lipo at all, but I’m saying it’s worth having that conversation, which I do with everyone, about the amount of liposuction you can do in that upper abdomen and what the potential consequences are.
So the next thing she wanted to talk about, just to kind of move along for the issue of time, is swelling. What can I expect for swelling? How long am I going to look big? How would you guys answer the questions? And what sort of things do you try to do to help with swelling after surgery?
Dr. Salvatore Pacella: Yeah, I think the swelling is a huge part of the postoperative recovery. I routinely tell patients to expect to be swollen for six months to a year afterward, in particular the distance or the anatomy or real estate between the belly button and the upper waistline area. That area is markedly swollen for months and months and months afterward, and it can also be numb.
And patients just really need the expectation of that. So oftentimes, for a good four to five weeks, I use an abdominal binder and compress that relatively snug and tight, and then after that time, I usually have them stay into some sort of compression garment for about three months that could be Spanx or really snug yoga pants that go all the way just below the bra line.
Dr. Sam Jejurikar: Sam, what about you?
Dr. Sam Rhee: Yeah, there’s a lot of swelling for a while, and I caution patients because I’ve had a couple of patients that went and saw a therapist without asking me and getting some sort of ultrasonic treatment or some other treatment and actually causing skin necrosis in the abdominal flap as a result of it.
And they’re just so hell-bent on dealing with the swelling on their own, what they want to do with it. And I just tell them, listen, you have to take your time with this. This is not a super-fast process like some other procedures are. So yeah, compression, that’s important, but also avoiding things that can actually be detrimental as well.
Dr. Sam Jejurikar: I have two questions for you guys. One, do you think drains are helpful in the minimization of swelling? And two, is there any point in time after surgery where you do feel comfortable with either Lymphatic massage or entomology or any other form of external treatment to help with swelling?
The Importance of Drains and Pain Management in Abdominoplasty
Dr. Salvatore Pacella: There has been a big push in plastic surgery to avoid drains and abdominoplasty, and I will say I just have not bought into that. A small patient with minimal fat, minimal dissection, thin amount of skin maybe could tolerate not having a drain, but it’s just such a large surface area to collect fluid, particularly the fact that you often get some of this exudate from the liposuction fluid that’s coming into the wound or the abdominal plastic subcutaneous space.
So I routinely use drains in everybody, and sometimes they’re in for weeks on end. It’s a challenge. I would usually say that for Lymphatic massage, I would probably give it a good six weeks before any of that kind of aggressive another manual Lymphatic massage I would recommend.
Dr. Sam Jejurikar: What about you?
Dr. Sam Rhee: I’m with Sal. I do quilting sutures and all that. But even with that, I still use drains on all my patients. I agree. The liposuction having all of that liposuction pubescence still there can play a role, especially for the initial. And I’m just conservative with it.
I don’t like being overly aggressive when I feel like the long-term consequences can be of issue. I’m also conservative. As I said, I’ve had a couple of bad experiences with patients going to see therapists for some sort of massage-type treatment, so I just tell them to hold off for about six weeks.
I think if you have a provider that you trust that you can work with, then as we’ve talked about with scar management, that’s one thing, but if you’re working with a variety of different people or you don’t know what they’re doing on my end, I will just be very conservative with it.
Dr. Sam Jejurikar: I really agree with that last point that you just made. Going to providers that you know and work with and can communicate with, I think, helps a lot. I’ll answer the second question for my first. I am a big fan of Lymphatic massage or entomology. I think the sooner they start it beyond the first ten days or so, I like it.
Personally, I think that the name of the game for me is getting this one to go away as quickly as possible. I feel like the less they can be stretched out afterward. When you’re dealing with patients that have poor skin elasticity, which is by definition a tummy tuck patient, I think the better the results are, so typically; I’ll start it; we do it through our center about ten or 14 days after surgery.
And I’m very happy with it. I haven’t noticed any wound healing complications that I would attribute to that relative to other factors. But yeah, I definitely would be on the lookout for that. And I agree with both of you guys on drains. I’ve kind of used drains at the beginning of my career. I went through a couple of years span where I tried not to use them at all. And I just thought the patients looked swollen and didn’t look as good.
Personally, I know there are people that get good results not using drains, but for me, because I’m so focused on swelling going down as quickly as possible, just like you guys, I like the drains. So she had one more concern, and that concern was, am I going to hurt after surgery? How long am I going to hurt for? And what are you going to do to try to make my pain better? How would you guys treat pain? What’s your standard protocol?
Dr. Salvatore Pacella: Well, just like we talked about several episodes ago, abdominoplasty…my prediction pain. It can be a painful operation, particularly when we’re talking about placation of the musculature. There are various options for treating pain at a local level. I think one of the most common things surgeons use is EXPAREL, which is an injectable Marcaine and injectable long-acting anesthetic.
Unfortunately, we don’t have it on the formulary at my health system. So instead, I use something a little bit more unique. It’s called a pain pump. It is two little tiny catheters that get sewn into the muscle repair. So I actually sew these catheters right at the level underneath the muscle repair, and they slip in and out very easily.
And then, at the end of the case, I hook this up to a big bulb, which the patient will carry around with them for about four days. And it’s got about 400 CCS of this long-acting anesthetic, which is just constantly being injected. And I have found that to be really nice because I think it really can do a huge job of taking the edge off the pain.
Dr. Sam Rhee: For me, I don’t use pain pumps, although I have in the past. It’s just one of those things that I found personally. They work. They definitely work. I just found them to try to encumber them. Yeah, just for me, as a solo practice guy to incorporate into my practice, just managing that. I have been experimenting with gabapentin, which I think has been very helpful for a lot of patients.
And that’s thanks to Sam. In our last episode, we were talking about postoperative pain management, and I do offer EXPAREL. I am of mixed feelings about it. I don’t know if you’re a big believer. I think you are, but you’ll tell me about it in a second. I’ve been pretty happy with injecting a lot of Marcaine at the end of the case and just sort of getting them by for the first couple of days.
They generally tend to do okay. It’s an up-charge for me for EXPAREL, and I’m okay with it. Maybe it’s just my own experience, or it’s like I said, it’s in my hands. It wasn’t something that I told every patient, listen, this is something that’s a game changer, but maybe I have to revisit it. I know you and a couple of other people have told me this is something that’s super helpful.
Dr. Sam Jejurikar: I think it’s helpful. I just think a pain pump is helpful. It seems to work great in some people and maybe not so great in others. I think we’ve had a lot of conversations about this sort of multimodal approach to treating pain. It’s another tool that you can use. I think gabapentin is a nice narcotic thing that we can use.
I’ve been using Celebrex More, which is and which is a non-steroidal anti-inflammatory, which is nice. I think our goal is to make people comfortable while minimizing the number of muscle relaxants and narcotic pain medications they’re on. But ultimately, it is going to hurt no matter what you throw at them. There is just no way to get rid of the pain.
And so those were her big concerns. Here are her postop results. I actually don’t have any pictures of the scar, which is ironic, given that we talked about it. So sorry about that, guys, but she had some pretty aggressive liposuction of the upper abdomen. I tightened her muscles all the way from stem to stern. Yeah, this is her about six months out.
Dr. Salvatore Pacella: Go back to the obliques if you can there, Sam. So I think a takeaway point here is just to look at the hourglass improvement he’s achieved here. I mean, that’s really substantial. It almost looks like you removed a couple of ribs.
Dr. Sam Jejurikar: No ribs were harmed during this case.
Dr. Salvatore Pacella: No, but I mean, that’s just a testament to really the placation and extra liposuction done on the lower back. Really good result.
Dr. Sam Rhee: Yeah, that’s what Sal said about that central portion of the abdomen making that sort of Holloway sort of look. That looks really nice. That looks natural. It looks really aesthetic.
Dr. Sam Jejurikar: Well, I think unless you guys have any other closing thoughts, I will continue to learn from you guys. And I just love going over these cases and seeing your guys approach things because I think if you’re doing general surgery, there’s really one way to take out a gallbladder.
But in plastic surgery, there are so many different ways to handle the same case, and so many different plastic surgeons get good results doing things differently that I continue to love talking to you guys and learning from you guys.
Dr. Sam Rhee: Exactly the same.
Dr. Sam Jejurikar: Well, thanks. Yeah, thanks, viewers, for watching yet another podcast. And until next time, have a great Sunday!
It is common for patients to negotiate an appropriate level of activity after undergoing tummy tuck, breast augmentation, liposuction, or any other combination of surgeries that make up a Dallas mommy makeover. The thought is, if they can convince me that they need less time to recover than other patients, somehow the surgery will be lessened in magnitude, or that they will be able to recover more quickly after the procedure.
Childbirth takes a dramatic toll on the female body. To reverse those changes with a mommy makeover, significant surgery is involved. With a Dallas tummy tuck (abdominoplasty), in addition to removing skin, extensive sculpting of the waist and upper abdomen is performed with liposuction, and the muscles of the abdominal wall are significantly tightened. Undue straining for a period of time after surgery can disrupt the sutures, and lead to a less then desirable postoperative result. In addition, straining after surgery can cause problems with wound disruption and bleeding, not to mention prolonged swelling in the abdomen, breasts, and lower extremities.
I usually recommend that my patients take 1-2 weeks off of work after surgery. Some patients will take less time and others more, depending on the level of physical exertion required at their work place. I also strongly advise my patients to refrain from any vigorous exercise for 6-8 weeks after surgery. Although it is important to walk almost immediately after surgery to prevent blood clots and respiratory problems, too much activity can lead to infection, bleeding, and wound healing problems.
Ultimately, to get the best result after mommy makeover, a patient has to allow herself the appropriate amount of time to recover. Should you have any questions, please do not hesitate to contact Dr. Jejurikar’s office at 214-827-2814.
Many patients who have lost massive amounts of weight come to the office inquiring about panniculectomy.They have been told by their friends or by other physicians that it is an equivalent operation to tummy tuck (abdominoplasty).
Panniculectomy does have some pleasing effects, but it is not the same thing as an abdominoplasty.With a tummy tuck, the excessive skin of the abdominal wall is removed, the belly button is reshaped, and the abdominal wall is tightened extensively.Oftentimes, liposuction is also performed with this to help provide the patient with a narrower waistline and a more pleasing figure.
Panniculectomy is a functional operation.Specifically, excessive skin located below the belly button is removed as a wedge resection.There is no significant undermining of the skin above the belly button, so patients are still left with a significant amount of redundant skin after this operation.In addition, the belly button is not reshaped, the abdominal wall is not re-tightened, and no liposuction is performed.
Both operations have significant uses, and there is a place for both, but it is important that patients understand the key differences between these procedures.
Should you have any questions about body contouring procedures, contact Dr. Jejurikar at 214-827-2814.
Virtually no patient comes to the office requesting a long scar.In fact, this is the major draw back to abdominoplasty (tummy tuck) surgery for most patients.
Although the scar cannot be eliminated with this operation, Dr. Jejurikar’s goal is to place it in as cosmetically acceptable position as possible.He asks his patients to wear either a bathing suit bottom or an undergarment they would like to be able to wear after surgery, and makes every attempt to design the incision to fall in this location.In addition, he attempts to close the scar as meticulously as possible, leading to as fine a scar as possible.Even with this, in some cases, the scars heal thicker and wider than desired. In these cases, topical medications or corticosteroid injections may be needed to improve the scar. In rare cases, a scar revision in which the scar is excised is required. In some patients, scarring must be treated aggressively for several months to 2 years after the procedure.
Should you have any questions regarding abdominoplasty, the location of the incisions, or scarring, please do not hesitate to contact Dr. Jejurikar at 214-827-2814.
Many patients come to the office inquiring about mini tummy tucks. The rationale behind this is quite clear. They would like a smaller scar, and believe that there is very little difference between a mini tummy tuck and a standard tummy tuck.
There are key differences between the operations. In a mini tummy tuck, there is very little separation of the skin from the abdominal wall muscles, meaning that less skin can be removed. In addition, there is usually no tightening of the abdominal wall muscles, particularly in the abdominal wall above the belly button. Therefore, if a patient has upper abdominal bulging or fullness, a mini tummy tuck doesn’t correct it. Finally, there is no reshaping of the belly button with a mini tummy tuck.
An advantage of a mini tummy tuck, however, is that, given there is less lifting of the skin from the abdominal wall muscle, liposuction of the entire abdominal wall and flanks can be performed much more extensively and much more safely. This is because there is less chance of wound healing complications.
Ultimately, mini tummy tucks are best for women that have undergone pregnancy and have only small lower abdominal pooches and only minimal to moderate changes to their abdominal wall. It also can be good for men who have lost large amounts of weight. For women that have bulging of the upper and lower abdomen with significant excessive skin and stretch marks, a full tummy tuck is almost always a better option.
Should you have additional questions, contact Dr. Jejurikar at 214-827-2814.
Many patients ask if their muscles truly need to be tightened during a tummy tuck. For most patients, the answer is yes. After pregnancy or massive weight loss, many women develop a condition known as rectus diastasis. With this condition, the midline vertical muscles that extend from the sternum and rib cage to the pubic bone, known as the rectus abdominis muscle, separate in the midline. This leaves a gap that was not present before pregnancy or weight loss. The gap is not indicative of muscle weakness, but it does lead to an abnormal bulge in the upper abdomen. As well, it can contribute to an overhanging skin apron in the lower abdomen.
Because this is not indicative of muscle weakness, performing abdominal wall exercises to strengthen the rectus muscles do not considerably improve this. The only true way to fix the abdominal bulging is to tighten these muscles by bringing them back together in the midline. As of now, this can only be accomplished with surgery, with the placement of multiple sutures to restore the overall integrity of the abdominal wall.
Obviously, removal of skin and reshaping the belly button are also integral portions of an abdominoplasty (tummy tuck). For most patients, however, failure to tighten the muscles of the midline abdominal wall would lead to less than optimal results.
For additional questions, please do not hesitate to contact Dr. Jejurikar via the web or via telephone at 214-827-2814.
Becoming a mother is a transformative experience, but the journey can take a toll on your body. Many women find that even with dedicated exercise and healthy eating, certain post-pregnancy changes to their body remain difficult to address. This is where a Mommy Makeover can help. Combining procedures tailored to restore a woman’s pre-pregnancy body—or enhance it further—a Mommy Makeover is one of the most sought-after cosmetic surgeries today. With Dr. Sam Jejurikar, a highly experienced and board-certified plastic surgeon at the Dallas Plastic Surgery Institute, you can achieve stunning, natural-looking results.
What is a Mommy Makeover?
A Mommy Makeover is a customizable combination of procedures designed to address the physical changes caused by pregnancy, childbirth, and breastfeeding. The most common areas of focus include the abdomen, breasts, and body contour. However, the specific procedures included depend on each patient’s unique goals.
Common components of a Mommy Makeover include:
Abdominoplasty (Tummy Tuck): Tightens abdominal muscles and removes excess skin, especially after multiple pregnancies. Dr. Jejurikar often incorporates multidirectional muscle tightening to achieve a flatter, firmer abdomen.
Breast Augmentation and/or Lift: Restores volume lost after breastfeeding and corrects sagging to create a youthful, lifted appearance.
Liposuction: Removes stubborn fat deposits resistant to diet and exercise, sculpting a more contoured silhouette.
Fat Transfer: Enhances curves, such as augmenting the buttocks or hips, using your own fat.
Additional procedures like labiaplasty or facial rejuvenation may also be included based on the patient’s preferences.
Dr. Sam Jejurikar: A Trusted Expert in Mommy Makeovers
Dr. Sam Jejurikar is a nationally recognized plastic surgeon known for his precision, artistry, and patient-centric approach. As a member of the prestigious Dallas Plastic Surgery Institute, Dr. Jejurikar combines advanced techniques with a personalized touch to deliver outstanding results.
Why choose Dr. Jejurikar for your Mommy Makeover?
Expertise in Complex Procedures:
Dr. Jejurikar has extensive experience in body contouring and breast surgery, two critical components of a Mommy Makeover. His expertise ensures optimal results tailored to each patient.
Focus on Natural Results:
With a keen eye for aesthetics, Dr. Jejurikar prioritizes creating natural, balanced results that enhance your body without appearing overdone.
Comprehensive Care:
From your initial consultation to post-surgical follow-ups, Dr. Jejurikar and his team are committed to providing compassionate, thorough care.
Cutting-Edge Techniques:
Dr. Jejurikar utilizes advanced surgical methods, such as VASER liposuction for enhanced fat removal and refined body contouring.
Benefits of a Mommy Makeover
A Mommy Makeover offers numerous physical and emotional benefits, including:
Restored Confidence: Regain your pre-pregnancy body—or an even better version of it—helping you feel confident and empowered.
Customizable Approach: Tailored to address your specific concerns, from sagging skin to stubborn fat.
One Surgery, Multiple Improvements: Combining procedures reduces overall recovery time compared to undergoing surgeries separately.
Long-Lasting Results: With a healthy lifestyle, the effects of a Mommy Makeover can be enjoyed for many years.
The Ideal Candidate for a Mommy Makeover
While every patient is unique, the ideal candidate for a Mommy Makeover typically:
Has completed their family or does not plan to have more children (additional pregnancies can reverse some of the procedure’s effects).
Maintains a stable weight and is close to their goal weight.
Is in good overall health with no medical conditions that could impair healing.
Has realistic expectations about the results.
Recovery and Results
The recovery process for a Mommy Makeover varies depending on the procedures included. Typically, patients can expect:
Initial Recovery: Most patients take 2-3 weeks off work and daily activities. You’ll need help with childcare and household responsibilities during this time.
Swelling and Bruising: These are common but subside significantly within the first few weeks.
Final Results: While initial results are noticeable soon after surgery, full results become apparent as swelling diminishes, usually around 3-6 months.
Dr. Jejurikar provides detailed post-operative instructions to ensure a smooth recovery and maximize your results.
Frequently Asked Questions
Q: How much does a Mommy Makeover cost?
A: Costs vary based on the procedures included. During your consultation with Dr. Jejurikar, you’ll receive a detailed quote tailored to your treatment plan.
Q: Can a Mommy Makeover address stretch marks?
A: While a Mommy Makeover isn’t designed to treat stretch marks specifically, a tummy tuck can remove skin affected by stretch marks in the lower abdomen. Stretch marks outside of this area may still remain.
Q: Can I combine a Mommy Makeover with other procedures?
A: Absolutely! Many patients add treatments like facial rejuvenation, labiaplasty, or fat transfer to complement their results.
Schedule Your Consultation with Dr. Sam Jejurikar
A Mommy Makeover can help you reclaim your body and confidence, empowering you to feel like the best version of yourself. With Dr. Sam Jejurikar, you’re in expert hands every step of the way. From personalized consultations to transformative results, his dedication to excellence ensures your journey is as rewarding as your outcome.
If you’re ready to take the next step, schedule your consultation with Dr. Sam Jejurikar at the Dallas Plastic Surgery Institute. Contact us today to learn how a Mommy Makeover can transform your life!
Contact
Contact
Our Location Dallas Plastic Surgery Institute
9101 N. Central Expwy.
Suite 600, Dallas, TX 75231
Tel: 214-827-2814